American Headache Institute
Head, Neck, & Facial Pain
Treatment Centers

Treatment
Treatment can not begin without a thorough
history and physical examination of the cervical spine
OUR EXAMINATION OUR RESEARCH SUPPORT
- We look where others do not – the neck.
- A safe, meticulous examination of the neck reveals pain
- Invasive testing such as x-ray, CT scan, MRI, or injections,
Call Us
(248) 841-1543

Thought of your neck?
We Have!
TREATMENT
M. Nordin, Dr Med Sc Assessment of Neck Pain and Its Associated Disorders: (359 articles reviewed, 95 admissible) “There was no evidence that specific MRI findings are associated with neck pain, cervicogenic headache, or whiplash
exposure. No evidence supports using cervical provocative discography, anesthetic
facet, or medial branch blocks in evaluating neck pain. There is support for subjective self-report in monitoring a patients’ response to treatment”.
(Spine 2008;33:4S,S1-S220).
For more than 3 decades, we have learned the most
insightful questions to ask, and the most relevant tests
to perform on your first visit. Our in-depth
series of historical questions often exposes
the cervical spines’ involvement. Our
highly specific, meticulously designed
examination of neck positions and subtle movements
is capable of bringing about a surprising decrease or
abolishment in head and facial symptoms.
The vast majority of new patients experi-
ence a significant alteration of their symp-
toms during the examination with over
40% reporting a complete abolishment. In as few as
1-3 visits, the role your cervical spine may play is best
answered when controlled repositioning of your neck
brings about significant changes in your symptoms.
P. Rothbart, MD, Medical Director, Rothbart Pain
Management Clinic, Toronto, Ontario..
“Approximately 800 new headache patients per year are examined at our clinic. An estimated 80% of these patients are diagnosed with cervicogenic headache. Of these patients almost none are referred with this diagnosis”.
“Physicians are not taught to consider or explore neck structures when investi-
gating headaches. This results
in a rarely diagnosed but common
condition”, says Dr. Rothbart.



As Dr. Nordin states above, there is scientific support for
“subjective self-report” by the patient in monitoring
symptom response during examination and treatment.
We invented an examination process for head and facial
symptoms which we call “Centralization Analysis”. It
relies on patient self-report.
Here’s How It Works
If
your symptoms
are coming from your neck,
the American Headache Institute
has discovered which symptoms will abolish first,
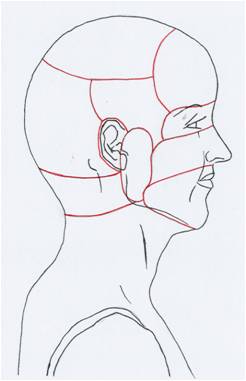
second, third, and so on, starting with zone 10 (mouth). We call this “Centralization”. Once all of your head and facial symptoms have been identified in the 10 symptom zones below, your cervical treatment program is aimed
at reducing and abolishing the symptom which is
farthest from your neck. Watching your face and
OUR EXAMINATION ADVANTAGE
A. Chorti, MSc The Prognostic Value of Symptom Response in the Conservative Management of Spinal Pain: “Only for changes in pain location and/or intensity with repeated spinal movement testing (Centralization) or in response to treatment did the data provide support for use of symptom response to inform management”.
(Spine 2009;34:2686-2699).
M. Werneke, MS, PT, Dip MDT A Descriptive Study of the Centralization Phenomenon: A Prospective Analysis “Categorization by changes in pain location to mechanical assessment and treatment allowed identification of patients with improved treatment outcomes and facilitated planning of conservative treatment of patients with acute back and neck pain syndromes”.
(Spine 1999;24:676-683).
head symptoms dissipate in a predictive,
predetermined, and orderly fashion, is
our unique clinical discovery and our big
treatment advantage. Together, we
observe your centralizing symptoms
which demonstrates the necks’
involvement and reassures us
that the treatment is both
correct and effective.
N. Bogduk, PhD Anatomy and Physiology of Headache: “Because of its prevalence, every physician has a responsibility to be able to assess headaches: either to identify headaches they can manage themselves, or those that require referral. Ultimately headache may require specialist investigation and management”.
(Biomed & Pharmacother 1995;49:435-45).
B. Mark, DDS Cervicogenic Headache Differential Diagnosis and Clinical Management: Literature Review. “The cervical spine must be evaluated to rule out cervical spine dysfunction with patients who have symptoms in the craniocervical-mandibular region”.
(J Craniomandibular Practice 1990; 8:332-38).
M. Gallagher, MD Cervicogenic Headache; A Special Report. “Evaluation of the neck, determining its role in the patient’s headache problem, establishing a working diagnosis and including the neck in the treatment plan, regardless of diagnosis, is the most helpful
for both patient and physician”.
(Neurotherapeutics 2007;7:
1279-83).
10
1
LAST
Suboccipital &
Upper Cervical
(Zone 1)
FIRST
Mouth
(Zone 10)
F. Antonaci, MD Diagnosing Cervicogenic Headache.
“Differential diagnosis is sometimes a challenge and kinematic (movement) analysis of neck motion may aid in diagnosing”.
(J Headache Pain 2006;
7:145-48).
For decades, physicians and dentists have known the cervical spine can refer pain into the head, jaw, and face. And until now, there was little known about how to treat such a neck problem. Focused exclusively on the neck, your treatment program is individually tailored in 4 specific areas;
OUR TREATMENT
Centralization of Head Symptoms
Order of Symptom Abolishment
S. Haldeman, MD, PhD, DC,
President, Neck Task Force Report
“Treatment involving exercise, manual therapy,
educational interventions, and patient self-efficacy
are more effective than alternative strategies for
patients with neck pain”.
(Spine 2008;33:4S,S1-S220)
OUR RESEARCH SUPPORT
(Direct Quotes)

